The literature commonly describes normal shoulder girdle alignment with the following criteria:
- Shoulder height lies slightly below the level of T1 and plumb line (Line of Appleton) runs central through the acromion
- Impaired alignment can manifest as elevation, depression (acromion below T2, AC joint lower than SC joint) or protraction
- Superior Angle of the Scapula at Spinal Level T2
- Inferior Angle of the Scapula at Spinal Level T7-T8
- Distance of Margo medialis from the Spine: 7,5cm / 3 in (~4 fingers)
- Scapula position: 30° anterior rotation to the frontal plane
Possible movements of the scapula are:
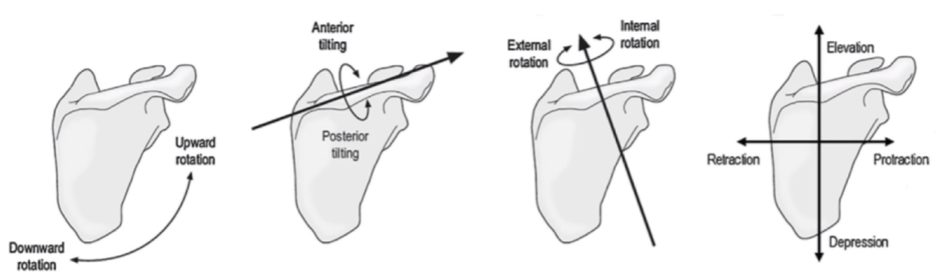
Muscles around the scapula:
Many muscles form so-called force-couples which means that their forces act together on a joint to produce rotation. These forces may actually exert pulls in opposite directions.
- Serratus Anterior + Trapezius pars descendens: Upward rotation
- Trapezius pars ascendens: Posterior tilting
- Trapezius pars transversus: Retraction
- Levator scapulae: Downward rotation + craniomedial translation
- Rhomboids: Downward rotation + Retraction
- Pectoralis minor: Downward rotation + anterior tilt
Deficiency or overactivity in one or more of these muscles can lead to an impaired alignment:
| Impaired alignment | Possibly shortened muscle(s) | Possibly weak and elongated muscle(s) |
| Downward rotated scapula (inferior angle more medial than superior angle) | Levator scapulae
Rhomboids |
Trapezius pars descendens
Serratus anterior |
| Scapular depression (lower than T2-T7 area) | Pectoralis major
Latissimus dorsi |
Trapezius pars descendens |
| Elevated scapula (superior angle above ACJ) | Levator scapulae | |
| Elevated scapula (superior angle + ACJ elevated) | Levator scapulae
Trapezius pars descendens |
|
| Entire scapular spine elevated | Levator scapulae
Trapezius pars desc. Rhomboids |
|
| Increased retraction (distance between medial border and spine <7,5cm) | Rhomboids
Trapezius pars desc. |
Serratus anterior |
| Increased protraction (glenoid oriented anteriorly, distance between medial border and spine > 7,5cm) | Serratus anterior
Pectoralis major |
|
| Winging Scapula / Scapula Alata (prominent medial border) | Subscapularis hypertrophy | Serratus anterior
Other: Hyperkyphosis, scoliosis |
| Scapular Tipping /Tilting (inferior angle lifting off of the thorax) | Pectoralis minor
Biceps brachii short head Coracobrachialis |
| Study | Reliability | Sn | Sp | LR+ | LR- |
| Ellenbecker et al. (2012) | Inter К= 0.16 -0.26 | NA | NA | NA | NA |
| Tate et al. (2009) | NA | NA | NA | NA | NA |
| Comment: Ellenbecker et al. (2012) distinguished between ‘normal’ and ‘scapular dyskinesis’ in 71 healthy uninjured baseball players. O’Leary et al. examined scapula posture Tate et al. (2009) demonstrate validity of scapula dyskinesis observation for less upward rotation, less clavicular elevation and and greater clavicle protraction in overhead athletes. |
|||||
![]()